Incident
Incident Overview Diagram
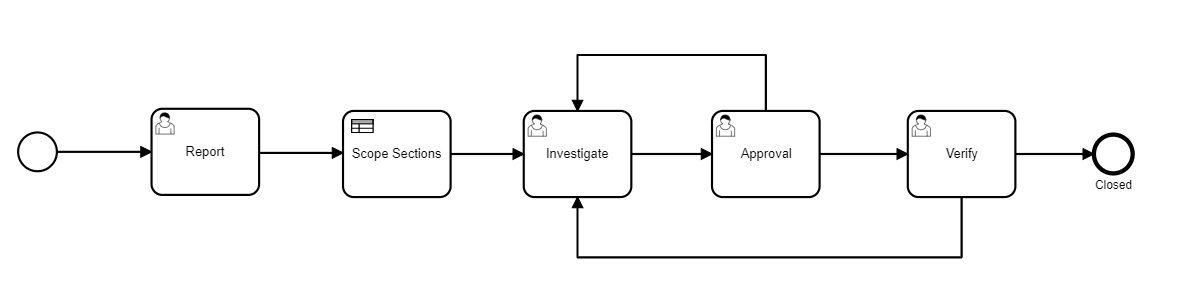

An out-of-the-box workflow of an Incident consists of these steps:
- Report
- Scope Sections
- Investigate
- Approval
- Verify
- Closed
Incident Form Sections
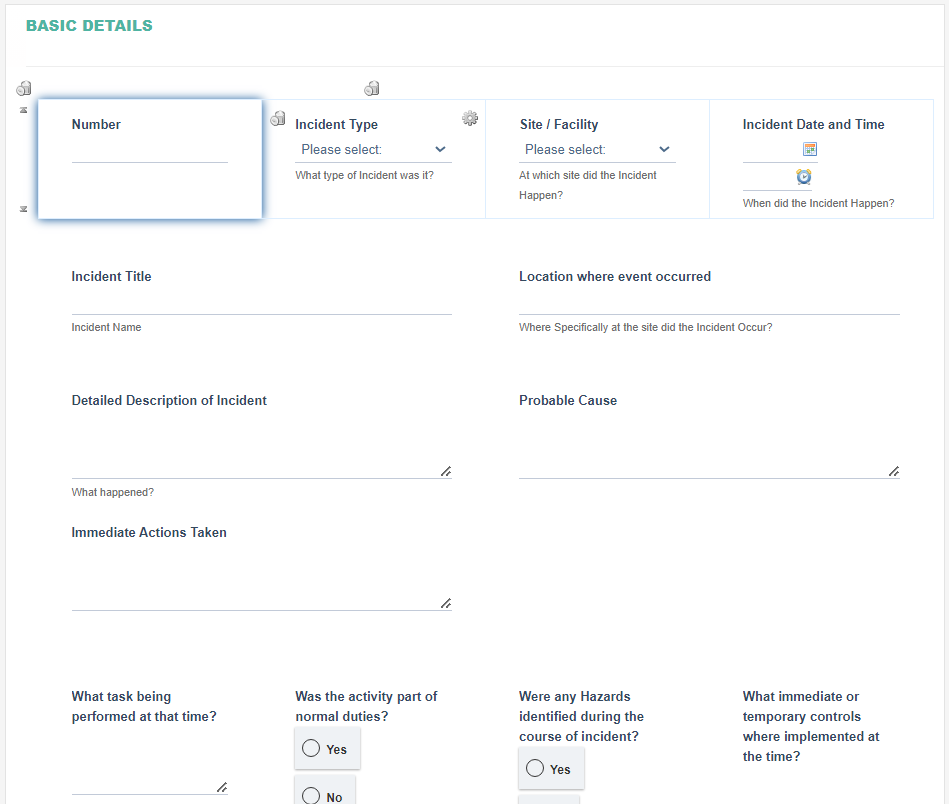
- Basic Details Section
|
Fields |
Field Explanation |
|
Number |
|
|
Type |
|
|
Site/Facility |
|
|
Incident Date and Time |
|
|
Incident Title |
|
|
Locations where event occurred |
|
|
Detailed Description of Incident |
|
|
What task was being performed at that time? |
Allow free text entry. Only shown when Incident Type = Other |
|
Was the activity part of normal duties? |
Allow Selection from Yes or No. Only shown when Incident Type = Other |
|
Were any Hazards identified during the course of incident? |
Allow Selection from Yes or No. Only shown when Incident Type = Other |
|
What immediate or temporary controls where implemented at the time? |
Allow free text entry. Only shown when Incident Type = Other |
|
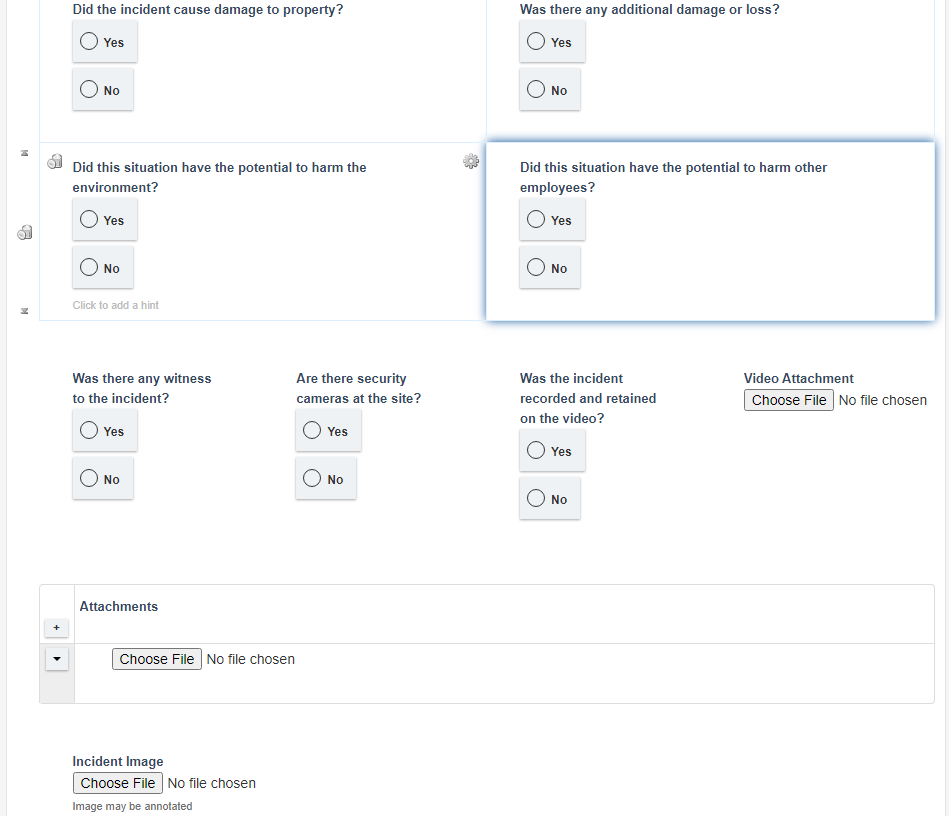
Did the incident cause damage to property? |
Allow Selection from Yes or No. Only shown when Incident Type = Other |
|
Was there any additional damage or loss? |
Allow Selection from Yes or No. Only shown when Incident Type = Other |
|
Did this situation have the potential to harm the environment? |
Allow Selection from Yes or No. Only shown when Incident Type = Other |
|
Did this situation have the potential to harm other employees? |
Allow Selection from Yes or No. Only shown when Incident Type = Other |
|
Was there any witness to the incident? |
Allow Selection from Yes or No. |
|
Are there security cameras at the site? |
Allow selection from Yes or No. If ‘Was there any witness to the incident’, selected as Yes then this field will be visible. |
|
Was the incident recorded and retained on the video? |
Allow selection from Yes or No. If ‘Are there security cameras at the site?’, selected as Yes then this field will be visible. |
|
Video Attachment |
Allow file selection. If ‘Was the incident recorded and retained on the video’, selected as Yes then this field will be visible. |
|
Attachment |
|
|
Incident Image |
|
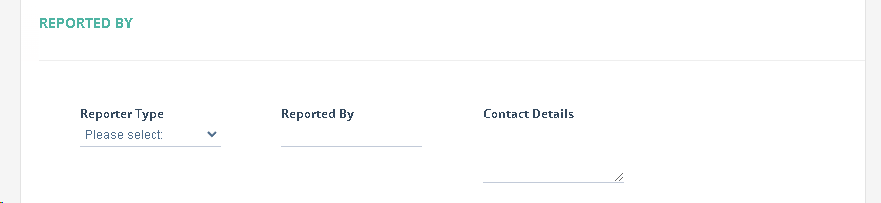
- Reported By Section
|
Fields |
Field Explanation |
|
Reporter Type |
|
|
Reported By |
|
|
Contact Details |
|
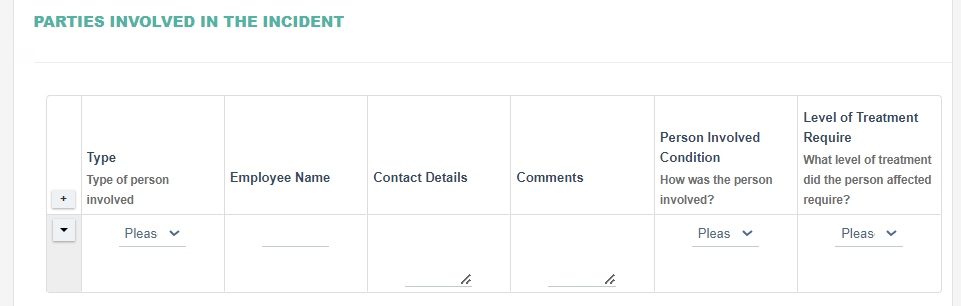
- Parties Involved in the Incident Section
|
Fields |
Field Explanation |
|
Type |
Allow selection from ‘Employee’, ‘Contractor’ and ‘Visitor’. |
|
Employee Name |
Allow free text entry. |
|
Contact Details |
Allow free text entry. |
|
Comments |
Allow free text entry. |
|
Person Involved Condition |
Allow selection from ‘Injured’, ‘Suffered Incident’, ‘Suffered Incident’, ‘Suffered Illness’, ‘Fatality’, and ‘Other’. |
|
Level of Treatment |
Allow selection from ‘First Aid’, ‘Medical Treatment (General Practitioner)’, ‘Medical Treatment (Special Practitioner)’, ‘Hospitalisation’ |
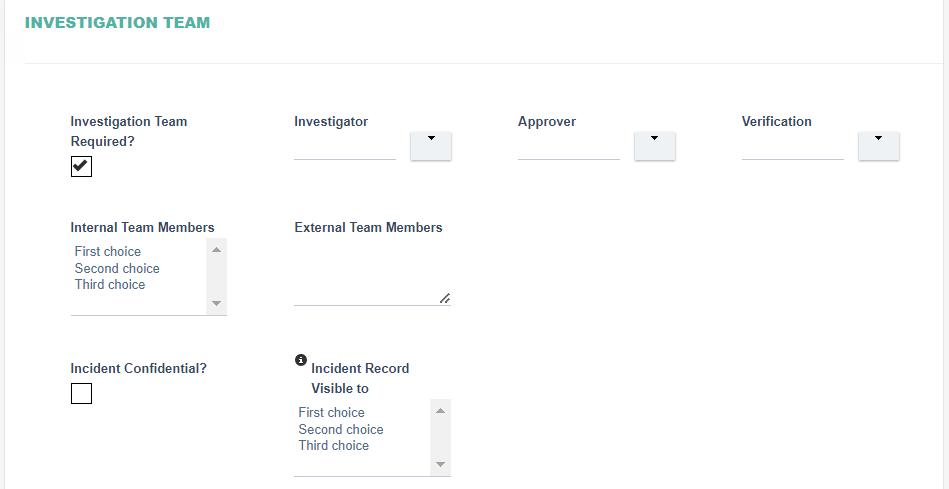
- Investigation Team Section
|
Fields |
Field Explanation |
|
Investigation Team Required? |
|
|
Investigator |
Allows selection from Users and Groups, this field is automatically set based on the Site / Facility. The Investigator is assigned to the Investigation step of the Workflow |
|
Approver |
Allows selection from Users and Groups The Approver is assigned to the Approval step of the Workflow |
|
Verifier |
Allows selection from Users and Groups The Verifier is assigned to the Verify step of the Workflow |
|
Internal Team Member |
|
|
External Team Member |
|
|
Incident Confidential? |
|
|
Incident Record Visible to |
|
- Injuries/Illness Details Section

|
Fields |
Field Explanation |
|
Show Body Map |
|
- Body Map Section
|
Fields |
Field Explanation |
|
Markup |
|
- Person Information Section

|
Fields |
Field Explanation |
|
Employment Type |
|
|
Name |
|
|
Job Title |
|
|
Contracting Company |
|
|
Date Hired |
|
|
Date of Birth |
|
|
Gender |
|
|
Employee ID# |
|
|
Address |
|
|
Phone #1 |
|
|
Phone#2 |
|
|
|
|
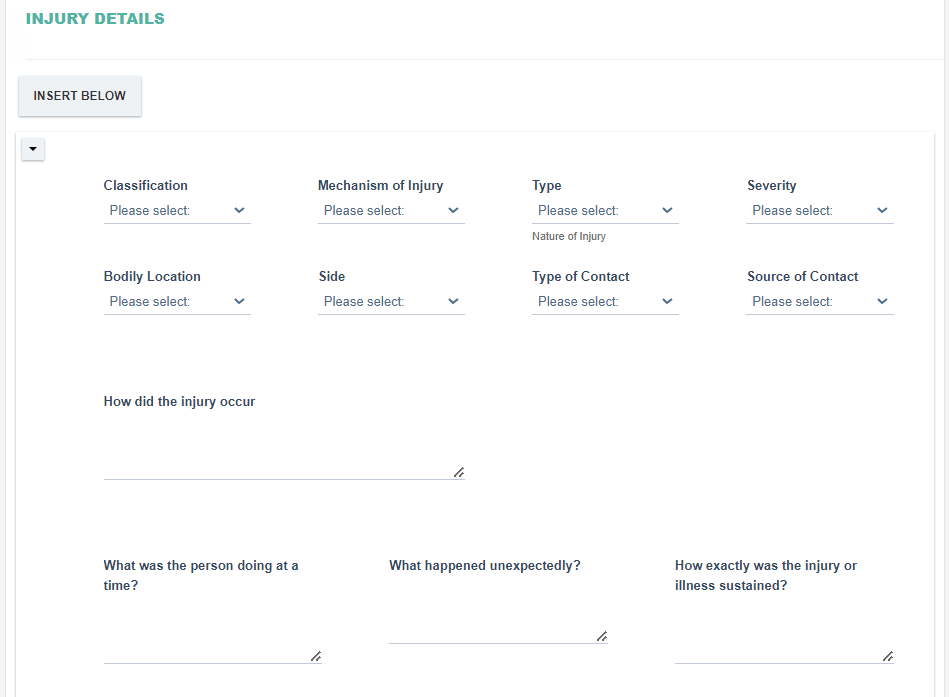
- Injury Details section

|
Field |
Field Explanation |
|
Classification |
Allow selection from Injury, Skin Disorder, Respiratory Condition, Poisoning, Hearing Loss and Other |
|
Mechanism of Injury |
Allow selection from:
|
|
Type |
|
|
Severity |
Allow selection from Disease, Fatality, First Aid, Medical Treatment and Other. |
|
Bodily Location |
|
|
Side |
Allow selection from Left, Right, Lower, Upper, Second, Third, Fourth. |
|
Type of Contact |
Allow selection from Caught between, Chemical, Cold environment, Cold Surface, Electricity, Mobile equipment and Noise. |
|
Source of Contact |
Allow selection from Movement, Buildings / Structures, Doors and Handling of material/equipment. |
|
How did the injury occur |
Allow free text entry. |
|
What was the person doing at a time? |
Allow free text entry |
|
What happened unexpectedly? |
Allow free text entry |
|
How exactly was the injury or illness sustained? |
Allow free text entry |
|
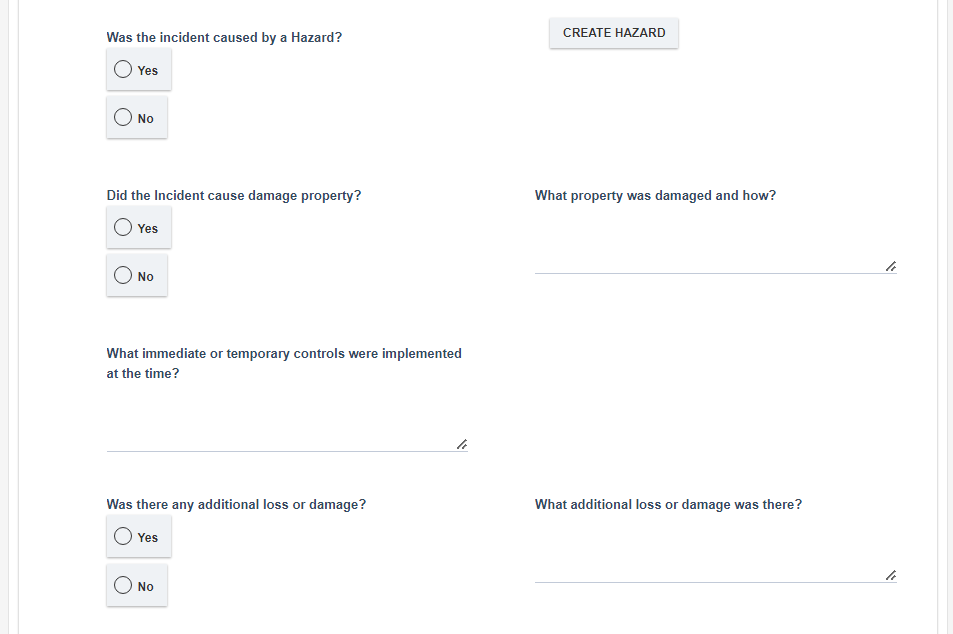
Was the incident caused by a Hazard? |
Allow selection from Yes or No |
|
CREATE HAZARD |
Creates a record in the Hazard Module |
|
Did the Incident cause damage property? |
Allow selection from Yes or No |
|
What property was damaged and how? |
Allow free text entry if the selection above is Yes |
|
What immediate or temporary controls were implemented at the time? |
Allow free text entry |
|
Was there any additional loss or damage? |
Allow free text entry |
|
What additional loss or damage was there? |
Allow free text entry if the selection above is Yes |
|
Did this situation have the potential to harm the environment? |
Allow selection from Yes or No |
|
How could the situation have potentially harmed the environment? |
Allow free text entry if selection above is Yes |
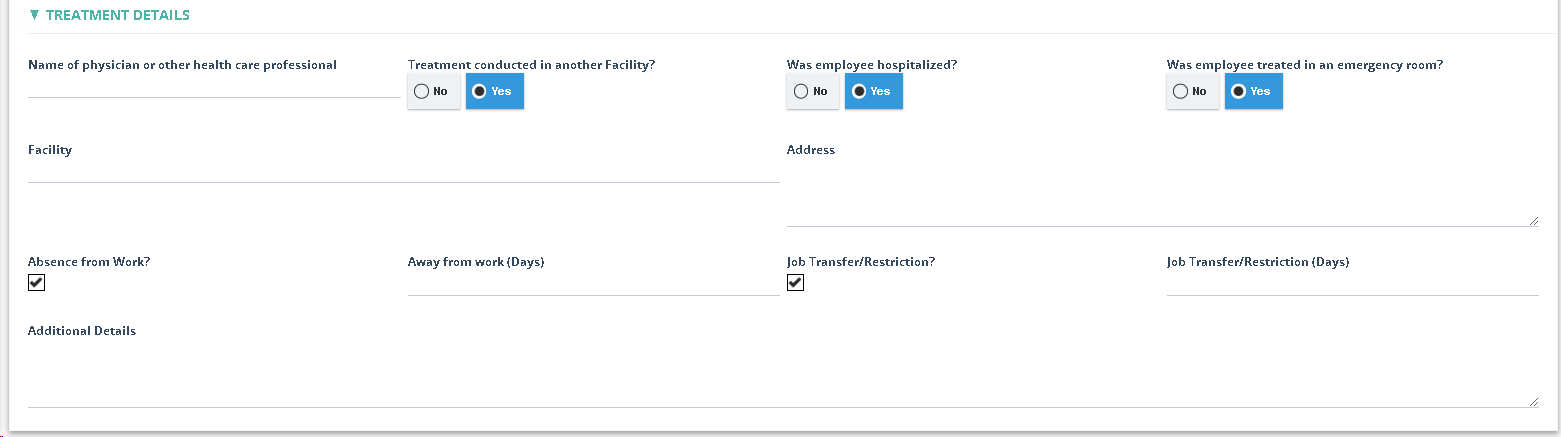
- Treatment Details section
|
Field |
Field Explanation |
|
Name of physician or other health care professional |
|
|
Treatment conducted in another Facility |
|
|
Was employee hospitalized? |
|
|
Was employee treated in an emergency room? |
|
|
Absence from Work? |
|
|
Facility |
|
|
Address |
|
|
Job Transfer/Restriction? |
|
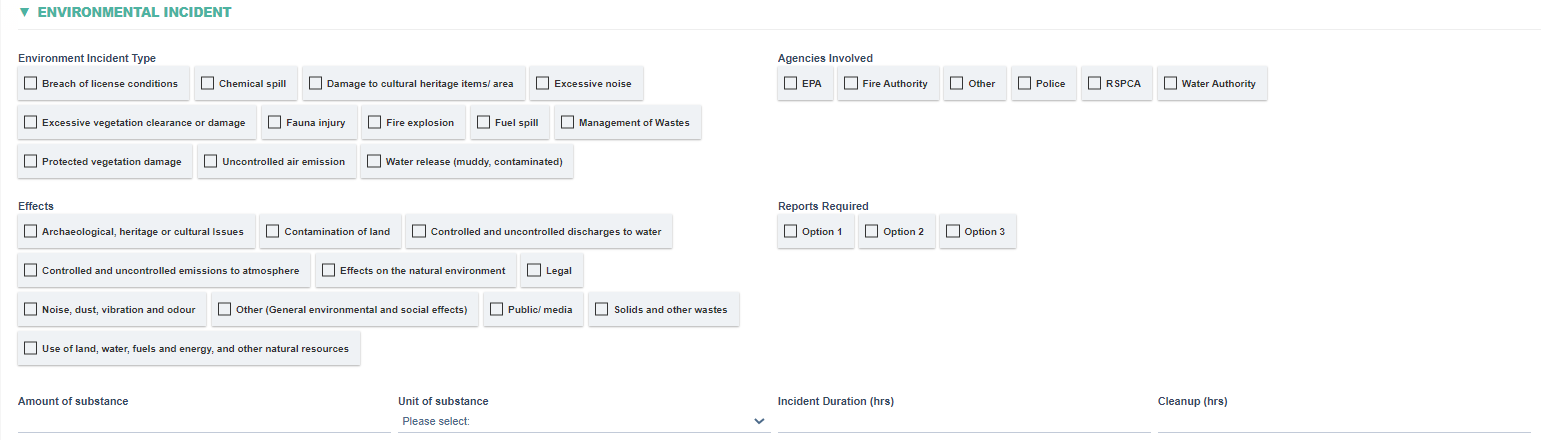
- Environmental Incident section
|
Field |
Field Explanation |
|
Environment Incident Type |
|
|
Agencies Involved |
|
|
Effects |
|
|
Reports Required |
|
|
Amount of substance |
|
|
Unit of substance |
|
|
Incident Duration (hrs) |
|
|
Cleanup (hrs) |
|
- Vehicle Incident section

|
Field |
Field Explanation |
|
Registration Number |
|
|
Vehicle Incident Type |
|
|
Vehicle Type |
|
|
Additional Details |
|
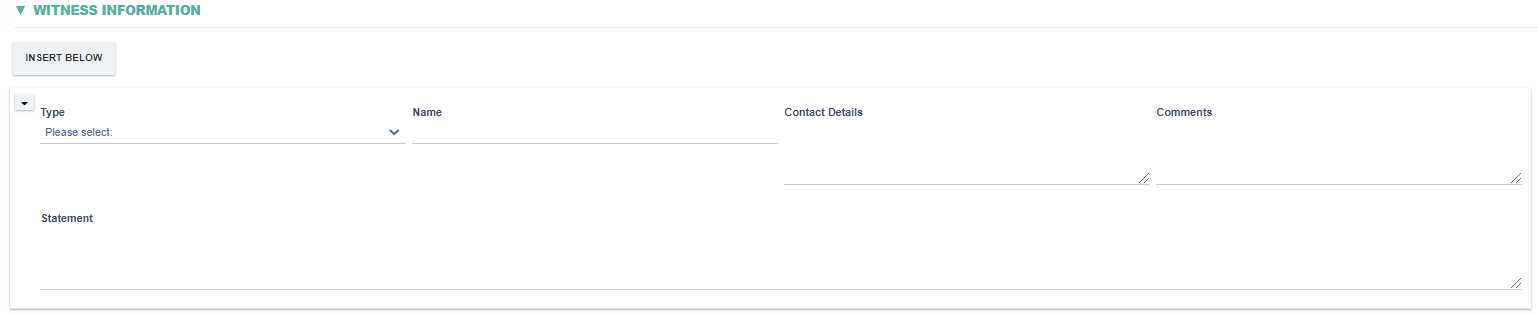
- Witness information section
|
Field |
Field Explanation |
|
Type |
|
|
Name |
|
|
Contact Details |
|
|
Comments |
|
|
Statement |
|
- Incident Impact section

|
Field |
Field Explanation |
|
Incident Severity |
|
|
Potential Breach of Safety Rules |
|
|
Is this Incident Reportable |
|
|
Conduct Risk Assessment |
|
- Sequence of Event section

|
Field |
Field Explanation |
|
Date and Time |
|
|
Who |
|
|
What |
|
|
Why |
|
- Incident Cause section

|
Field |
Field Explanation |
|||||||||||||||||||||||||||||||||||||||
|
Has Incident Cause been determined? |
|
|||||||||||||||||||||||||||||||||||||||
|
Attachments |
|
|||||||||||||||||||||||||||||||||||||||
|
Immediate Cause |
|
|||||||||||||||||||||||||||||||||||||||
|
Secondary Cause |
|
|||||||||||||||||||||||||||||||||||||||
|
Additional Details |
|
|||||||||||||||||||||||||||||||||||||||
|
Lessons Learnt |
|
- Action Plan section


|
Field |
Field Explanation |
|
Actions Required? |
|
|
ACTION PLAN |
|
|
START ALL ACTION |
|
- Cost

|
Field |
Field Explanation |
|
Item |
|
|
Cost |
|
- Verification

|
Field |
Field Explanation |
|
Incident actions completed as planned |
|
|
Additional Details |
|